As part of our work in the field of value-based health care, BCG has developed a method of assessing a country’s readiness to take this approach to improving health and lowering health care costs.
Improving Value-Based Health Care
- Meeting the Data Challenge
- Assessing a Country’s Readiness
- From Concept to Reality
- Leveraging Data to Refine Treatments and Improve Outcomes
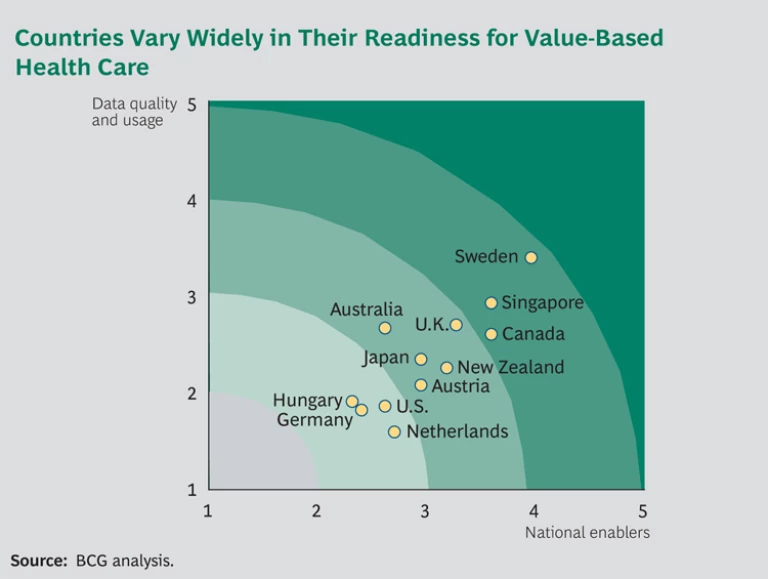
The method evaluates country readiness along two key dimensions. The first is the degree to which a country has key enablers in place—for example, common national standards and IT infrastructure, national legal and consent frameworks, the ability to link health outcomes with costs, and high engagement on the part of clinicians and policymakers. The second dimension is a country’s existing registries or other health-data repositories, both in terms of the richness and quality of their data and the sophistication of the medical community’s use of the data across 12 critical disease areas.
So far, we have assessed the readiness of the health systems in 12 countries: Australia, Austria, Canada, Germany, Hungary, Japan, the Netherlands, New Zealand, Singapore, Sweden, the U.K., and the U.S. The exhibit below ranks these countries on the two dimensions described above. As the exhibit illustrates, when it comes to implementing value-based health care, Sweden is the most advanced country on our list, followed closely by Singapore, whereas Hungary and Germany have the furthest to go.
Our analysis of country readiness has also identified some common themes around which countries tend to cluster. For example, some countries, such as Hungary, face basic capability gaps that limit progress on both dimensions. They need to get the basics in place in order to progress. In other countries, a single national health-care infrastructure exists, but the engagement necessary to guide the definition of appropriate metrics or to support their adoption is missing. We find this to be the case in Japan and the Netherlands.
In other countries, the fragmented nature of the national health-care system has seriously limited the collection and use of national health-outcomes data. In addition to the U.S., where this is a widely acknowledged problem, it is also the case in Germany.
Some countries, like Austria and New Zealand, have the core capabilities in place and are collecting quality data, but they need to resolve one or two major obstacles or create new incentives in order to push data collection further. Others have some world-class registries that operate according to best practices, but these practices need to be replicated across all of the country’s health-data repositories. Australia, Canada, and the U.K. are examples of countries in this category. And still others collect comprehensive and reliable data but lack the analytical capabilities required to use the data effectively to improve clinical practice. We find this to be the case in Singapore.
Finally, there are the rare countries that have advanced outcomes-based data collection that is actively used by an engaged clinical community and that has delivered national benefits in the form of improved health outcomes. This is the case in Sweden, as described in detail in this report.