I t’s a secret hiding in plain sight. The $7.6 trillion global health care sector has a value problem. Despite decades of efforts to control spending, costs continue to rise at roughly double the rate of GDP growth in most developed countries. That is putting severe pressure on health care budgets and, in many countries, is leading to rationing in the form of longer wait times or restricted access.
It would be one thing if those spending increases were delivering commensurate improvements in patient health. But that is far from the case. There are wide variations in health outcomes across hospitals, regions, and countries, with no clear causal relationship between money invested and health
In response to these problems, some industry leaders have begun to embrace a model known as value-based health care. According to this approach, the primary objective of any health system should be continuous improvement in health outcomes for a given level of cost. (See “The Basic Principles of Value-Based Health Care.”) Value-based health care is a promising model for the reorganization of care. We believe it has the potential to deliver substantially improved health outcomes at significantly lower cost than health systems are currently able to achieve. Realizing that potential, however, will require significant changes in behavior on the part of stakeholders throughout the health system.
The Basic Principles of Value-Based Health Care
Value-based health care makes the delivery of improved health outcomes for the same or lower cost the primary objective of global health systems. The approach is founded on the systematic measurement of health outcomes and of the costs required to deliver them for clearly defined sub populations—for example, all patients who suffer from a given disease or condition, such as type 2 diabetes, or who share a similar risk profile, such as the multimorbid elderly. Teams of clinical specialists use this outcomes and cost data to develop customized interventions to improve the ratio of outcomes to costs for each patient group over time.
By aligning industry stakeholders around the shared objective of improving health care value, value-based health care has the potential to deliver substantially improved health outcomes at lower costs than most health systems around the world are currently able to achieve.
The approach also improves access to appropriate care, defines relevant innovations in treatment and care delivery, and provides major new business opportunities for health care organizations in both the public and private sectors.*
* For a comprehensive discussion of value-based health care, see Michael E. Porter, “What Is Value in Health Care?” New England Journal of Medicine, December 23, 2010; and “Value in Healthcare: Laying the Foundation for Health-System Transformation,” World Economic Forum, April 2017.
In particular, it will require much higher levels of cooperation. Specialists in key disease areas need to agree on the most important outcomes to measure. Providers need to work more closely with patients and patient advocacy groups to help achieve the outcomes most important to them. Clinical specialists at different points along the treatment pathway need to come together in interdisciplinary teams to create more integrated and customized interventions. And payers will need to work closely with providers, drug companies, and medical-device manufacturers to develop the most cost-effective modes of treatment.
In this respect, value-based health care is, first and foremost, a behavioral challenge. Meeting that challenge will not be easy. Health care is far too complex an industry for leaders to mandate the necessary cooperation or rely on the standard tool box of managerial techniques—new processes, organizational structures, and incentives—to make it happen. They need a smarter approach to behavioral change, one that is simultaneously simpler and more effective, to cut through the Gordian knot of increasingly complex health systems, unleash the energy and engagement of their people, and align their organizations around the shared goal of patient value.
Value-Based Health Care is, first and foremost, a behavioral challenge.
One place to start is with an approach to understanding and influencing behavior that BCG has developed in its work with leading business organizations around the world. We call it smart

Behavior may not be the only factor affecting an organization’s performance, but it’s an especially important one in highly complex industries such as health care. How people act, interact, and make decisions often spells the difference between high performing organizations and the rest. Seen from this perspective, human behavior is “performance in the making.”
The conventional approach to managing people’s behavior at work is, in effect, to tell them what to do. Managers use traditional organizational mechanisms such as reporting relationships, formal processes, detailed rules and guidelines, and key performance indicators (KPIs) to dictate how employees should behave. They reward them for compliance with those rules, processes, and KPIs and punish them for noncompliance.
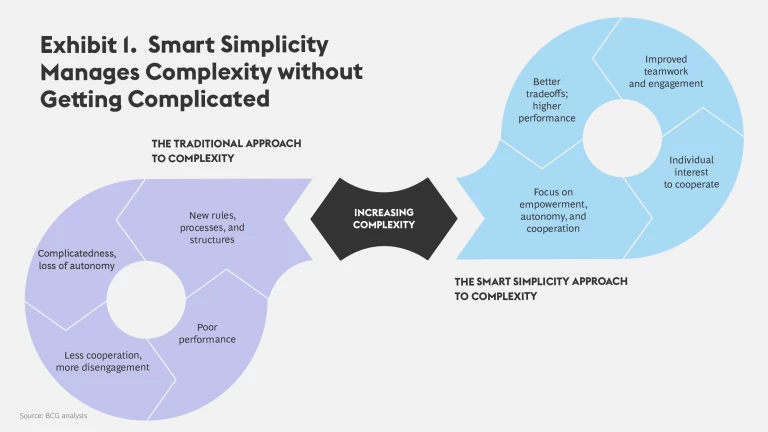
In modern work environments characterized by increasingly complex tasks and multiple (and sometimes conflicting) performance requirements, this approach is less and less effective. The more goals and objectives multiply, the more the rules, processes, and guidelines proliferate in an effort to manage complexity and control what people do. The paradoxical result is added and unnecessary layers of organizational complicatedness on top of necessarily complex tasks. Increasingly complicated organizations restrict autonomy and make it more difficult, not less, for people to work together to manage complexity.
Combining Autonomy and Cooperation. One of the principles of smart simplicity is that the more complex work becomes, the more the key to effective performance is to encourage autonomy, not restrict it. Autonomy is the freedom to exercise one’s judgment in the completion of a task. In situations where the task is simple and the goals clear, autonomy isn’t really necessary; the organization can create a rule or an algorithm that people can follow. But in situations where individuals and teams need to make tradeoffs among multiple objectives or multiple ways of achieving them, all the rules in the world cannot dictate the most appropriate solution for the specific situation. The only way to manage a growing number of increasingly complex tradeoffs is to give people the autonomy to exercise their judgment.
But autonomy alone is not enough. The more complex the work environment, the less likely that any one individual or group will have all the answers. Rather, people, teams, and entire organizational units need to work together to get to the best result. It’s therefore also essential for an individual’s autonomy to be deployed in the service of cooperation with others.
Cooperation may sound like a feel-good term, a self-evident value in any organization. That’s not how we’re using it. In reality, cooperation is a complex social process, hard to create and easy to destroy. The fact is, many people avoid cooperating if they can get away with it, and they will often use whatever autonomy they have to do so. Why? Because to truly cooperate with others requires people to bear the cost of necessary adjustments to their own goals for the greater good of the organization. Cooperation involves tension, the confrontation between different but equally valid perspectives and priorities, and sometimes considerable conflict. (Indeed, absence of conflict is often the first sign that cooperation isn’t taking place.) The challenge, therefore, is to find ways to make cooperation and the adjustments it imposes on people’s goals not only a worthwhile organizational objective but also a rational strategy for individuals.
Avoiding Complicatedness. Smart simplicity is the art of creating work organizations that manage complexity by combining autonomy and cooperation without adding complicatedness. (See Exhibit 1.) The approach is based on two key principles about organizational behavior that have come out of the social sciences. The first is that all human behavior is strategic. People behave the way they do in order to meet their individual objectives or goals, leveraging the resources available to them and working around the constraints. In this respect, human behavior is always rational. There are always “good reasons” for why people do what they do—even when, if viewed from the perspective of the organization and its goals, their behavior appears irrational or dysfunctional. Effectively shaping behavior requires understanding those reasons and knowing how to influence them to the ends of the organization.
The second principle is that, while leaders can’t directly control people’s behavior, they can shape the organizational context, the goals, resources, and constraints to which that behavior is a response. The way to effectively influence behavior in situations of high complexity is to create a context that unleashes the autonomy necessary for creative problem-solving and that, at the same time, makes it rational—a winning personal strategy—for people to harness that autonomy in the service of cooperation.

Smart simplicity is relevant to any industry, but it is especially relevant to health care. Few work environments today are subject to as much complexity as those in health care. Rapid advances in biomedical science have led to an exponential increase in the understanding of health and disease and in new tools to diagnose and treat patients. But they have also led to increased specialization, more-complex clinical decision making, and a concomitant fragmentation of care, which can make it difficult for providers to work together to take a truly integrated approach to patient health. The paradox of specialization is that it makes cooperation more necessary even as it makes it more difficult to
Complexity in health care is exacerbated by the industry’s many stakeholders. Payers, providers, drug makers, and medical device companies are separate but interdependent members of an increasingly intricate ecosystem. So are institutions that are not typically thought of as members of the health care industry—for example, university research labs, patient advocacy groups, and public-health organizations. All these various organizational entities contribute to patient care, but diverging goals and interests can make it difficult to create alignment around shared goals.
Like many businesses, health care has also witnessed a proliferation of new performance requirements in recent decades. Increasingly, clinicians are asked not merely to treat the patient and cure disease but also to control costs, maximize capacity utilization, minimize wait times, and ensure patient satisfaction, among other important goals. Multiple performance requirements further increase the complexity of the task.
The problem is made even worse by the way health care organizations have tried to manage rising costs and complexity. Much like managers in other industries, health care leaders have put in place more and more standardized processes, rules, guidelines, and KPIs. This growing complicatedness has significantly eroded the professional autonomy that clinicians used to enjoy while, at the same time, making it even more difficult for them to work together to make the tradeoffs necessary to deliver value to patients.
GROWING COMPLICATEDNESS HAS ERODED THE PROFESSIONAL AUTONOMY CLINICIANS USED TO ENJOY.
Consider the typical approach to cost control. Payers try to control costs by imposing constraints on medical decision making and patient choice in the form of utilization reviews, drug formularies, prior authorization, restricted provider networks, rationing, and the like. In response, many provider organizations focus on process efficiency, imposing top-down performance measures to increase their control over clinical practitioners.
It’s an understandable impulse. But the result is that highly qualified and experienced clinicians end up feeling micromanaged, caught between the demands of payers to contain costs, of hospital administrators to maximize the use of expensive medical technologies, and of themselves as professionals to provide the best treatments to their patients.
Clinicians still have the responsibility for making life-and-death decisions. But they are increasingly subject to bureaucratic controls that erode their capacity to exercise their own expertise and judgment in the best interest of their patients. The stress of bearing that distinctive emotional burden, with less and less control over the outcome, often leads to frustration, cynicism, and mistrust. No wonder the health professions have some of the highest levels of dissatisfaction and burnout. 2 At its worst, this situation can lead to a culture of blame in which poor performance or breakdowns are blamed on others rather than being occasions for reflection and continuous improvement.
The only way to cut through this dysfunctional complexity is to create organizations that give autonomy back to caregivers and channel it toward new kinds of cooperation across medical dis- ciplines and the different sectors of the health care industry. The basic idea behind value-based health care is to align industry stakeholders around the shared objective of improving measurable health outcomes delivered to patients for a given cost and then to give those stakeholders the autonomy, tools, and accountability they need to meet that objective.
How might health care leaders use smart simplicity to address the behavioral challenge of improving health care value? One useful place to begin addressing that question is with the phenomenon of outcomes variation.
In recent years, researchers have become aware of the wide- spread variation in the health outcomes delivered to patient groups across providers, countries, and regions within
Diabetes is a serious chronic disease that is reaching near- epidemic proportions. According to the International Diabetes Foundation (IDF), roughly 415 million adults suffered from diabetes in 2015—and nearly half of those cases went
In addition to this widespread human suffering, diabetes rep- resents a growing economic burden. Treatment for diabetes and related complications currently accounts for about 12% of global health care spending. IDF estimates that diabetes-related health expenditures will increase from $673 billion in 2015 to $802 billion in 2040. What’s more, the lion’s share of the costs associated with the disease is incurred treating patients with serious complications, which makes prevention and progression control critical to both delivering good health outcomes and minimizing the costs of care.
COMPARING OUTCOMES: THE US AND SWEDEN
The incidence of diabetes and the costs of diabetes care vary widely across national health systems. (See Exhibit 2.) Take, for example, the differing rates of type 2 diabetes in the US and Sweden. According to IDF, the age-adjusted prevalence of type 2 diabetes in the US adult population is 10.8%; in Sweden, the equivalent number is less than half as large—
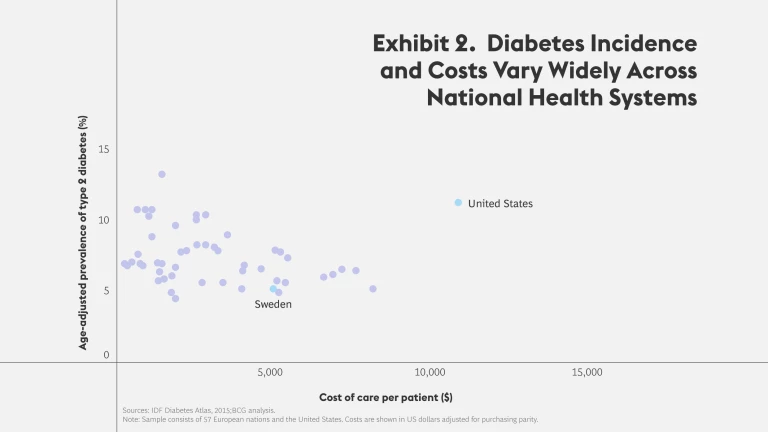
Because complications drive the lion’s share of costs, the higher complication rate in the US helps explain why the annual cost per patient of type 2 diabetes treatment in the US is double that in Sweden
HOW BEHAVIOR DRIVES VARIATION IN OUTCOMES
What explains these differences in health outcomes? Although genetic differences in the populations of the two countries probably account for some of the variation, the main causes are behavioral. Diabetes is largely a lifestyle disease, so patient behavior in terms of diet and exercise plays a central role in its prevalence and
Another key behavioral driver is the way in which the health systems in the two countries treat diabetes. To analyze the behavioral roots of different approaches to clinical practice in the two countries, we reviewed the scientific literature and interviewed clinical experts and representatives of patient groups. Our goal was to develop a high-level behavioral map of how the two systems typically diagnose and treat diabetes. While there are, of course, exceptions in both health systems and our analysis is not comprehensive, we identified two important clusters of behavioral difference.
Individual- Versus Team-Based Approach to Care. In the US, individual physicians typically take responsibility for diabetes care. The vast majority of type 2 diabetes patients (roughly 80%) are treated by their primary-care physician (PCP). It’s rare for PCPs to refer diabetes patients to an endocrinologist unless the case is especially serious—and when they do, the specialist tends to take over primary responsibility for the patient’s care.
In Sweden, by contrast, clinicians take a more interdisciplinary, team-based approach. A patient’s general practitioner (GP) usually makes the initial diagnosis, but that diagnosis immediately triggers the involvement of a variety of other experts, who play different but complementary roles. For example, most primary-care facilities in Sweden have specially trained, full-time diabetes nurses on staff who play a central role in diabetes care (we’ll describe that role in more detail below). In the US, by contrast, diabetes nurses work mainly in secondary-care treatment facilities, not primary care. Therefore, they tend to see only the most seriously ill patients.
In Sweden, clinicians take a team-based approach to care.
Swedish GPs also refer diabetes patients to specialists (known as diabetologists, a term used in Sweden to describe endocrinologists who specialize in diabetes care) far more frequently than US primary-care physicians do. But that does not mean those patients stop seeing their GP. Rather, Swedish diabetes patients move easily between health care providers in the system, from GP to diabetes nurse to specialist and back again in a way that does not happen routinely in the US.
Finally, Swedish primary-care centers often appoint one GP to serve as the designated diabetes “node.” In addition to treating his or her own patients, the node oversees the care and disease progression of other diabetes patients in the center, plays a consultative role with his or her colleagues, and, in general, helps coordinate the movement and care of patients among the multiple caregivers on the interdisciplinary team.
Treating Symptoms Versus Treating Behaviors. Another major behavioral difference between the two systems is that the clinical interventions around diabetes in Sweden tend to be far more holistic than in the US. Whereas US clinicians focus primarily on medical measures—diagnosing symptoms and then prescribing drugs or performing procedures to address them— Swedish clinicians balance this approach with the kind of educational and behavioral interventions that are critical for managing a lifestyle disease such as diabetes.
These differences are partly a function of how much time primary-care physicians spend with their patients. Once diagnosed, diabetes patients in the two countries visit their doctor with about the same frequency—roughly three or four times a year. But the time they spend per visit differs substantially: between 5 and 10 minutes in the typical US office visit, compared with 15 to 20 minutes in Sweden. The additional time that Swedish doctors spend with patients creates more opportunities to educate them on the behaviors needed (such as proper nutrition and exercise) to manage their disease effectively. By contrast, because US doctors are more time constrained, they are forced to focus on the most immediate and acute effects of the illness, reinforcing the overreliance on medical measures to the relative neglect of educational and behavioral interventions.
The holistic interventions of the Swedish system are reinforced by that country’s team-based approach to diabetes care. Here, the role of the diabetes nurse is key. As soon as a general practitioner makes the initial diagnosis, he or she refers the patient to a diabetes nurse, who conducts an initial one-hour visit to develop a tailored plan and daily routine for managing the disease (including when to take medication and how to measure blood sugar). Diabetes nurses meet regularly with patients in followup appointments, where they examine their feet for signs of neuropathy or foot ulcers (key symptoms of disease progression), make any necessary appointments with specialists such as podiatrists or ophthalmologists, and in general help with the ongoing management of the disease.
In Sweden, the role of the diabetes nurse is key.
The presence of diabetes nurses in most primary-care settings also makes it easier for the system to focus its educational efforts not only on patients who have been diagnosed with diabetes but also on those at risk of developing the disease in the future. In other words, the Swedish approach contributes to prevention, not just to treatment and cure. And in general, it seems to integrate the traditionally separate domains of health care and public health better than the US system does.
Even specialists take a broader approach to diabetes care in Sweden. Diabetologists typically focus on the more serious cases, just as endocrinologists in the US do. But in some Swedish counties (roughly the equivalent of US states and the primary funders of health care), they also offer an intensive four-day program of examination and education for early-stage type 2 diabetes patients, in which they develop a comprehensive treatment plan and then refer the patient back to his or her general practitioner for followup. This practice helps slow down the progression of the disease.
HOW ORGANIZATIONAL CONTEXT SHAPES INDIVIDUAL BEHAVIOR
It may be tempting to explain these differences in behavior in terms of differences in the national or medical culture of the two societies. But that would be to beg the question, “Why have these different cultures led to different behaviors?” Looking more closely, we can identify specific aspects of the organizational con- text of the two health systems that have shaped those behaviors and to which those behaviors are a rational response.
Fee-for-Service Versus Capitation. Perhaps the most visible difference is the way in which caregivers are compensated for their work. Despite many changes in recent years, most US clinicians continue to be paid according to some version of the traditional fee-for-service model. In Sweden, by contrast, payment for primary care is usually based on capitation adjusted for a primary-care center’s population mix.
The US fee-for-service model helps explain why primary-care providers in the US are less likely than their Swedish colleagues to refer patients to an endocrinologist. If a large share of referred patients end up returning to that specialist for their ongoing care, the primary-care provider loses the patient and the associated revenue stream. Fee-for-service compensation also encourages US clinicians to focus on medical interventions, which are most likely to be reimbursed by payers. From the perspective of smart simplicity, these behaviors aren’t signs of irrational behavior or poor priorities. They are simply rational responses to the context in which people work. Changing their behavior requires changing the context.
A capitation-based incentive system, by contrast, encourages autonomy by making it easier to choose from a wider variety of interventions without having to get payer approval. As a result, more time and attention go to activities such as patient education. Capitation also gives Swedish clinicians an interest in preventing diabetes and minimizing its progression, because the fewer the cases, the lower the costs and the more the primary-care facility will be able to keep within its county-approved budget.
Comprehensive Outcomes Data. But capitated payments alone do not explain Sweden’s distinctive approach to diabetes care. A far more fundamental difference in the organizational context of the two health systems is that Swedish clinicians have access to comprehensive data on the health outcomes of diabetes patients nationwide. Since 1996, Sweden’s National Quality Registry for Diabetes (known by its Swedish acronym, NDR) has collected comprehensive outcomes data on more than 5 million Swedish diabetes patients. Since 2002, NDR data has been available online, allowing individual clinics to easily compare their own results with national statistics. NDR is one in a network of more than 100 such quality registries in Sweden, covering the majority of national health expenditures. These registries have become powerful engines of behavior change for clinicians and help explain why Sweden often ranks near the top in international comparisons of health
Because Swedish clinicians have data on the actual health outcomes they are delivering, they are empowered to identify the most effective treatment options and change their behavior accordingly. And because this data is publicly available to providers, payers, and patients, clinicians have an interest in cooperating with peers to improve their outcomes over time. Finally, access to comprehensive outcomes data ensures that the incentives associated with capitation work in the way they are supposed to: improving overall health care value rather than, for instance, becoming a perverse incentive that encourages undertreatment.
Some regional US health systems (for example, Kaiser Permanente) have active diabetes registries, which they use to identify best practices in care much as Swedish clinicians do. Until recently, however, there was no national US diabetes registry, and the new Diabetes Collaborative Registry is still in the early stages of
“Integrator” Roles. A third aspect of the Swedish organizational context for diabetes care is the explicit roles that have been created to support the team-based and holistic clinical approach. The diabetes nurse who is a central player in diabetes care and the general practitioner who is the designated diabetes node in a primary-care center are both examples of what we call “integrator” roles—actors with an interest in encouraging cooperation who help each member of the organization benefit from the cooperation of others. It is the existence of these clearly defined roles in overall care delivery that helps make Sweden’s approach to diabetes care so effective.
An Organizational Context That Delivers Value. Our analysis suggests that the combination of capitated reimbursement, the systematic measurement of health outcomes, and effective integrator roles make it easier for Swedish clinicians to work together to deliver value to diabetes patients. Put in the language of smart simplicity, these factors make cooperation an effective behavioral strategy for Swedish clinicians, and that is one of the reasons why Sweden has a much lower prevalence of type 2 diabetes than the US.
There is no reason why the US health system—or any health system, for that matter—couldn’t foster an organizational context that encourages comparable behaviors. In fact, some US providers have begun to do just that. A number of leading diabetes-focused clinics in the US— for example, the Joslin Diabetes Center in Boston—take a team-based approach to care that is quite similar to the Swedish model, and these specialty clinics provide some of the best diabetes care in the world. They are the exception, however. And even they struggle with aspects of the overall US health system (for instance, the continuing dominance of fee-for-service reimbursement) that function as disincentives for interdisciplinary cooperation among care providers. In other words, the challenge remains: how to spread the team-based model to the entire US health system.
The best US diabetes clinics take an approach that is similar to the Swedish model.

How might health care leaders go about creating organizations that combine autonomy and cooperation on the part of care givers to improve health care value? BCG’s work on smart simplicity has identified “six simple rules” for doing so. (See Exhibit 3.) The first three are designed to give people autonomy at work. The last three are designed to give them an interest in cooperation so that they willingly use their autonomy to work together toward the organization’s goals. Consider how the leaders at the university hospital of a major academic medical center used these rules to redesign the hospital’s operating model.

1. UNDERSTAND WHAT YOUR PEOPLE REALLY DO
The starting point is to analyze the behavioral dynamics that underlie an organization’s performance—much as we did in the previous section with the causes behind outcomes variation in diabetes care in the US and Sweden. The university hospital was a prestigious institution. It had a storied history of clinical innovation and drew patients from throughout its home country and even from abroad. More recently, however, the hospital had been struggling with a series of seemingly intractable performance problems.
Like many hospitals, the organization suffered from a nursing shortage. The problem had become so acute that a substantial percentage of beds were left empty for lack of nurses to staff them. The empty beds were wreaking havoc with the institution’s capacity utilization, causing it to post recurring budget deficits. Wait times for surgery and other critical procedures had also lengthened beyond legally mandated limits.
The hospital had tried a variety of interventions to address its capacity and cost problems. It had engaged in multiple rounds of belt-tightening, instituted “lean” initiatives to improve process efficiency, and put in place a variety of dedicated task forces to address specific issues like bed assignment. But these efforts in- variably foundered when it came to implementation. The organization’s inability to solve its problems damaged staff morale (making it even more difficult to recruit leading clinicians and experienced nurses) and was beginning to erode the hospital’s reputation.
A closer look at the hospital’s functioning revealed an even more disturbing trend: a steady erosion in the quality of care. To be sure, the hospital had world-class doctors and many areas of genuine clinical excellence; its staff treated some of the most complex cases in modern medicine. But the hospital was finding it more and more difficult to translate that excellence into the consistent delivery of quality health outcomes to patients. An analysis that tracked the hospital’s performance on commonly accepted health outcomes in ten major categories of care, ranging from heart disease to diabetes to cancer, found that in only one out of ten areas was the hospital above the national average in more than half the metrics. And on a comprehensive national quality ranking, the hospital came in last among its country’s university hospitals.
The institution’s leaders analyzed the behavioral dynamics underlying this poor performance. Instead of focusing on what people didn’t do, they focused on what they did do, why those behaviors made sense given the hospital’s organizational context, and how they contributed to the breakdowns in performance. Three behavioral patterns turned out to be especially important:
- Optimizing the Unit, Not the Hospital. Like most hospitals, this one was organized into departments according to medical specialty. Many of these units had strong reputations and, therefore, a lot of institutional power and professional pride. They controlled their own budgets, managed their own wards, set their own KPIs, trained their own students, and evaluated and promoted their own personnel. But they had become so good at optimizing their own performance that they would often do so at the expense of the hospital as a whole.
Take the hospital’s empty-bed problem. For the institution’s leaders, this was a massive constraint on the hospital’s ability to meet its budget. Yet, from the perspective of the specialty wards, empty beds were a resource. It was a typical ward practice to set aside beds so they would always be available for patients of the ward’s own doctors. So when the emergency room called, looking for a bed for a patient in need of further care, staff in the specialty ward would claim that no beds were available. In addition to creating unnecessary conflicts among units, this behavior exacerbated the hospital’s capacity utilization problem and long wait times. As one division head put it, “Everyone is focusing on the tents, but nobody is focusing on the circus.”
- Focusing on Process, Not Patients. Another set of behaviors had to do with how the individual units were being managed. One consequence of the hospital’s preoccupation with its financial problems was a proliferation of new guidelines and KPIs designed to help it meet its annual budgets. This led to an overwhelming management focus on process compliance and short-term budget targets—with limited attention to the impact on patients and health outcomes.
Clinicians, of course, cared about doing the best for their patients. But at the end of the day, their managers were judged on whether or not the unit was hitting its budget targets; they had neither the incentive nor the tools to find out in detail what kind of outcomes their clinicians were delivering to patients. The overreliance on financial and process metrics helped explain why the hospital’s quality of care was eroding. It also led to considerable tension between managers and clinicians and a lot of disengagement, especially on the part of junior clinical staff, who often felt there was little consideration of how the latest cost-cutting initiatives might be affecting quality. This tension was a factor in the high turnover the hospital was experiencing, which worsened the hospital’s nursing shortage and, therefore, its capacity utilization problem.
- Cumbersome Decision Making and Poor Implementation. The independence of the individual units and the exclusive focus on process compliance and short-term budget targets contributed to a third behavioral dynamic at the hospital: cumbersome and ineffective decision making. Because clinicians in one unit were never confident that other units had their best interests at heart, everyone wanted to be involved in every decision, leading to time-consuming meetings. And because everyone was involved, no one was really accountable—especially when decisions had implications for multiple units. As a result, new initiatives didn’t get implemented, it was difficult to take a holistic and integrated approach to patient care, and the lack of alignment (sometimes verging on mistrust) among the hospital’s leaders was becoming a major obstacle to innovation and continuous improvement. When division heads were asked to name their greatest fear as leaders, the most common response was “being accused by peers of having made a mistake.”
These were the behavioral dynamics that the hospital had to change in order to address its performance problems. The challenge was how to do it.
2. REINFORCE INTEGRATORS
One of the basic principles of value-based health care is that the key unit of analysis is the population of individuals who suffer from the same disease or condition or who share similar risk profiles. By focusing on distinct population segments, providers can meaningfully compare health outcomes, identify the causes of unnecessary variations in those outcomes, learn more about the clinical interventions that improve health outcomes for a given segment, and drive the systematic improvement of care over time. This population-based approach can be challenging for many health care organizations to implement because it cuts across the traditional functional structure of most care delivery networks.
The simple rule to “reinforce integrators” can be an effective way to address this problem. Integrators are individuals or work units that rely on cooperation to get their work done. Reinforcing them means giving them sufficient power to influence the behavior of others in the interest of greater cooperation. One example of the reinforcement of integrators is the central role played by diabetes nurses and diabetes nodes in the treatment of type 2 diabetes in Sweden. At the university hospital, creating new integrator roles became a key part of the transformation strategy.
To make it easier to focus on improving health care value, the hospital decided on a fundamental change in its operating model. Instead of organizing around medical specialties, it would organize around the patient. Specifically, the hospital identified a few hundred distinct patient groups based on disease, condition, or risk profile, each with its own characteristic treatment pathway and mix of required specialists and expertise. These groups were aggregated into a smaller number of patient areas characterized by similar treatments and clinical experts, and then further clustered within a handful of broad medical “themes” (for example, maternal and children’s health, cardio-vascular disease, cancer, and aging). These became the main organizational units at the hospital, with primary responsibility for managing beds and assigning nurses.
To focus on improving health care value, the hospital changed its operating model.
To animate this new organizational structure and make it function effectively, the hospital created an important new leadership role: the patient group manager. These managers are senior clinicians with deep experience in a specific treatment pathway ( juvenile rheumatoid arthritis, say, or congestive heart failure). They are responsible for designing a holistic, integrated approach to treatment and for coordinating the interdisciplinary teams of specialists who care for patients with the particular disease or condition. They develop and track appropriate outcome metrics, manage resources and budget, and drive improvements in value over time.
The patient group managers are integrators in the sense that their role is to orchestrate the cooperation needed from the interdisciplinary team that delivers care. For example, the patient group manager convenes a steering committee consisting of representatives from all the key medical specialties that play a role in caring for the patient group in question, as well as from related managerial units (such as IT) and patient advocacy groups. The committee responsible for the rheumatoid arthritis treatment pathway, for instance, includes a rheumatologist, physiotherapist, occupational therapist, nurse, and other clinical players, as well as a controller, a business development expert, and a patient representative. The idea is to give the relevant stakeholders a seat at the table so they can all contribute to developing a holistic approach to treatment for patients with the condition.
The patient group manager is not only a catalyst for more effective cooperation. He or she also enables increased autonomy on the part of the clinical staff. Instead of being micromanaged, the managers and their interdisciplinary teams have room to maneuver and the freedom to develop the best means of achieving the clinical and financial goals of the hospital.
3. INCREASE THE TOTAL QUANTITY OF POWER
There is a lot of talk these days about empowerment in modern organizations. Power is really the capacity of one person to make a difference on issues that matter to someone else. Increasing the total quantity of power is akin to increasing the number of cards in a deck. The greater the number of cards, the greater the variety of moves that each player can make. In the same way, expanding people’s behavioral options mobilizes them to find ways to satisfy the multiple requirements of a complex task.
Organizing around patient treatment pathways went a long way toward allowing the university hospital to take a more holistic approach to care delivery. But no hospital can be organized entirely around patient segments. At an academic medical center such as this one, medical specialists will always be central to delivering cutting-edge diagnostics and treatments and training the next generation of clinical experts. And there will always be some specialty functions that cut across all patient groups—for example, the emergency room, the operating room, the intensive care unit, the diagnostic laboratory, and the imaging department. This university hospital has retained these traditional functions, but by increasing the total quantity of power, it has reshaped how their staff interact with the patient group managers and with each other.
Personnel from the specialty functions continue to report to their functional managers. But the patient group managers, who are now key actors in multiple treatment pathways, have a formal say in performance reviews of those experts. Have the radiologists from imaging, for example, contributed to our ability to improve health outcomes in a cost-effective fashion? Have they been good team members, engaging in effective cooperation? In effect, by giving the patient group managers influence over the career progression of specialists, the hospital has increased the quantity of power that those managers have at their disposal to encourage effective cooperation.
At the same time, the specialists have a say in evaluating the performance of the patient group managers. Are they using our specialty resources wisely, maximizing their impact on patient health outcomes? Are they open to new ideas or innovations that we propose to leverage our expertise and resources? Are they providing the right kind of training opportunities for our new specialists? Instead of just responding to requests for their services, medical specialists are now in a position to influence how care is designed and delivered across a broad cross-section of treatment pathways. Their total quantity of power has been increased, as well as that of the patient group managers. As a result, interactions within the treatment pathways and among the specialty functions are becoming more constructive and more aligned.
4. INCREASE RECIPROCITY
In complex environments where organizations are pursuing multiple (and sometimes competing) goals, it’s critical to develop “rich objectives” that reflect the complexity of those goals and that acknowledge the tradeoffs necessary to achieve them. Rich objectives tend to increase the sense of reciprocity among actors—the mutual conviction that they have a shared interest in cooperation and that each actor’s success depends on the success of others.
The goal of improving health care value—defined as the ratio of outcomes to costs for a given disease, condition, or population segment—is one such rich objective. It has the potential to align all stakeholders around a common goal, to give clinicians a way to address issues of cost within the context of their core mission, and to create a common frame of reference for the all-important dialogue among payers, providers, and suppliers about payment. The challenge is to translate that goal into granular objectives that inform people’s day-to-day work.
As part of its new governance model, the university hospital has developed a balanced scorecard that includes KPIs in four key areas: quality of care delivery; productivity and financial performance; research, education, and innovation; and staff engagement and morale (including retention of key personnel). Patient group managers and their teams track their own performance across all four categories and meet monthly to discuss how they are doing and how they can improve; they are evaluated on how well they do, not in any single area but as a whole. The approach increases reciprocity among team members. Even more important, their senior managers track and are evaluated on the exact same metrics, increasing reciprocity and alignment across the managerial-clinical divide.
5. EXTEND THE SHADOW OF THE FUTURE
One of the biggest challenges in tracking health outcomes and improving them over time is the fact that the actual impact of a given treatment or procedure may not be apparent until years afterward. Therefore, another way that organizations can encourage cooperation is to extend the shadow of the future. They can do this by creating feedback loops that force clinicians to take into account the long-term impacts of their decisions on outcomes and costs.
Such feedback loops are increasingly being incorporated into new payment mechanisms known as value-based bundled payments. In Sweden, for example, the Stockholm County Council (the public entity responsible for funding health care for the roughly 2 million residents of the greater Stockholm metropolitan area) has piloted value-based bundled payments for hip and knee replacement. The approach holds providers financially responsible for the full cycle of care, including all diagnostics, any nonacute complications related to the primary surgery, and all patient-reported outcomes for up to two years after the operation. Because this payment model encourages clinicians to keep a longer timeframe in mind, they try hard to minimize costly reoperations due to complications and to consider the likely impact of their decisions on rehabilitation. In the first two years of the program, complications decreased by 18%, reoperations decreased by 23%, and revisions fell by 19%. What’s more, costs per patient declined by 20% and patient sick leave by 17%.
One new practice that is extending the shadow of the future at the university hospital is the more frequent rotation of clinical staff among different units at various points along the treatment pathway. For example, nurses who traditionally worked exclusively in an in-patient setting now routinely rotate into out- patient settings. This gives them a richer understanding of the challenges facing patients after they leave the hospital and of how decisions made earlier in their care can lead to better outcomes years after treatment.
6. REWARD THOSE WHO COOPERATE
Mechanisms to extend the shadow of the future create direct feedback loops that can have an immediate impact on behavior. But sometimes the tasks and activities are such that feedback can only happen indirectly, through the judgments and evaluations provided by others. In any organization, this is the role of management, and health care is no exception. From the perspective of smart simplicity, the central role of management is to encourage and reward cooperation—by making transparency, innovation, and ambitious aspirations the best choice for individuals and teams.
The university hospital is still in the middle of its transformation. The new operating model is placing new demands on the institution’s leaders, particularly those who run the specialty functions that previously held the lion’s share of power. But despite the fact that the new operating model is not yet fully implemented, the shift in the organization’s culture is palpable. Clinicians are learning how to use their new-found autonomy constructively and are working more closely together in interdisciplinary teams. Both managers and clinicians are increasingly being held accountable not just for costs but for the actual value delivered to patients. New roles like that of the patient group manager and new practices such as frequent rotation are making possible new career paths with more opportunities for professional development. Most important, performance is starting to improve. In the past two years, the hospital has operated without a deficit and has improved its ranking on the national quality index from last among university hospitals to third.
The BCG Henderson Institute is Boston Consulting Group’s strategy think tank, dedicated to exploring and developing valuable new insights from business, technology, and science by embracing the powerful technology of ideas. The Institute engages leaders in provocative discussion and experimentation to expand the boundaries of business theory and practice and to translate innovative ideas from within and beyond business. For more ideas and inspiration from the Institute, please visit
Featured Insights
.